What is Gastroesophageal Reflux?
Gastroesophageal reflux (or acid reflux) occurs when the stomach contents reflux back up into the esophagus and/or mouth. Reflux is a normal process that occurs in healthy infants, children, and adults. Most episodes are brief and go unnoticed.
Acid reflux becomes Gastroesophageal Reflux Disease (or GERD) when bothersome symptoms develop or injury to the esophagus occurs.
The amount of acid reflux required to cause GERD varies from person to person. In general, damage to the esophagus is more likely to occur when:
- Acid refluxes from the stomach back up into the esophagus frequently,
- When the reflux is very acidic, and
- When the esophagus is unable to clear the acid in a timely fashion.
GERD
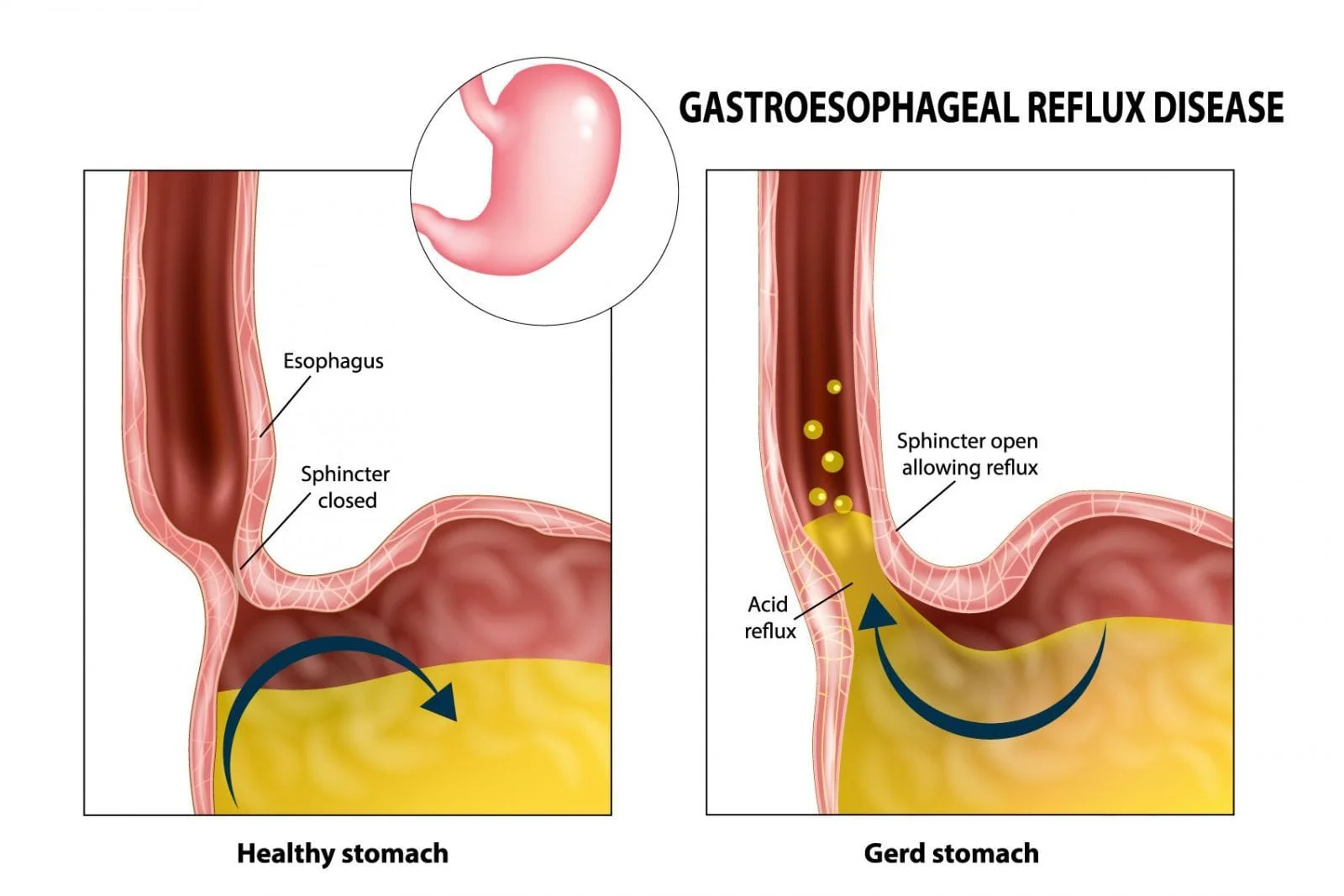
When we eat, food is carried from the mouth to the stomach through a muscular, tube-like structure known as the esophagus. In adults, the esophagus is approximately 10 inches long and 1 inch wide. It is a muscular tissue that expands and contracts to carry food to the stomach through a series of wavelike movements called peristalsis.
At the lower end of the esophagus, there is a circular ring of muscular tissue known as the lower esophageal sphincter (or LES). This muscle relaxes after you swallow to allow food to enter the stomach. Once the food enters your stomach it then contracts (or closes) to prevent food and acid from backing up into your esophagus.
If the LES becomes weak or is relaxed because your stomach is over-distended, liquid in the stomach can wash back up into your esophagus. This happens occasionally in all of us and typically does not cause any symptoms; however, if symptoms routinely occur this is known as GERD.
How common is GERD?
Quite common. Heartburn, one of the most common symptoms of GERD, is estimated to affect 10 million adults in the United States on a daily basis.
What are the symptoms of GERD?
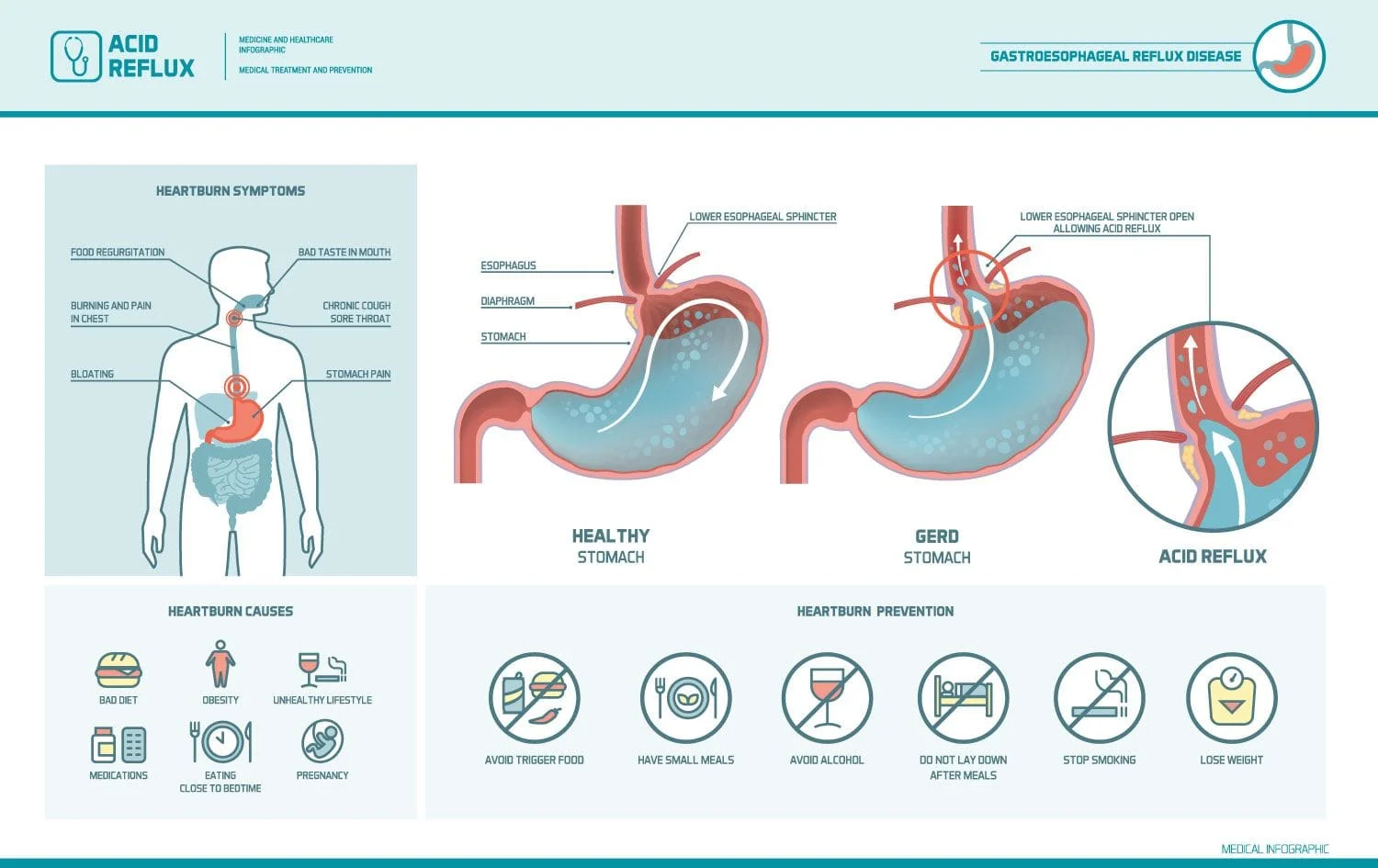
Symptoms may include:
- Heartburn or a burning sensation in the center of the chest, which sometimes spreads to the throat,
- Burning chest pain,
- An acid taste in the back of the throat,
- Regurgitation of foods or liquids,
- Nausea and/or vomiting.
- Stomach pain
- Non-burning chest pain
- Difficulty swallowing or food getting stuck
- Painful swallowing
- Persistent hoarseness
- Persistent sore throat
- Chronic cough, new onset asthma, or asthma only at night
- The sensation of a lump in the throat
- Worsening dental disease
- Recurrent lung infections or pneumonia
- Chronic sinusitis and
- Waking up in the middle of the night with a choking sensation
The following signs and symptoms may indicate a more serious problem, and should be evaluated by a trained medical professional immediately:
- Chest pain,
- Difficulty swallowing or painful swallowing
- Food getting stuck
- Choking
- Unexplained weight loss
- Vomiting up blood,
- A change in bowel habits
- Dark-colored stools
- Fevers, chills, sweats,
- Lightheadedness, dizziness
- Anemia
How is GERD diagnosed?
It is important to rule out potentially life threatening conditions that could be causing your symptoms. Chest pain can be a symptom of heart disease. If you have chest pain or any other alarming symptoms go to your nearest emergency department for immediate care.
A comprehensive history and physical exam will help Dr. Sinha and our medical staff to diagnose your condition.
Acid reflux can often be diagnosed based upon your symptoms and an appropriate response to a trial of medication. If you have symptoms of acid reflux but no evidence of complications or more serious disease, a trial of lifestyle modifications and medication may be recommended prior to more invasive testing.
Specific testing is required however when the diagnosis is unclear or if you have more serious signs or symptoms.
One or more of the following tests may be recommended to make a definitive diagnosis of GERD:
- Upper endoscopy or EGD — This is a procedure performed under mild anesthesia where a small, flexible tube with a light source and camera is passed into your esophagus, stomach and the first part of your small intestine or duodenum to assess for disease and changes in the lining of your esophagus, stomach, or duodenum. Biopsies can be taken during the procedure to assist with the diagnosis.
- 24-hour esophageal pH study — This test directly measures the acidity in your esophagus. A thin tube with a small device that measures the pH in your esophagus is inserted through your nose and into your esophagus. It is left in your esophagus for a period of 24 hours during which your will be asked to keep a diary of your symptoms. Afterwards, the data received will be analyzed to determine if the frequency of your reflux and pH readings recorded correlate with your symptoms.
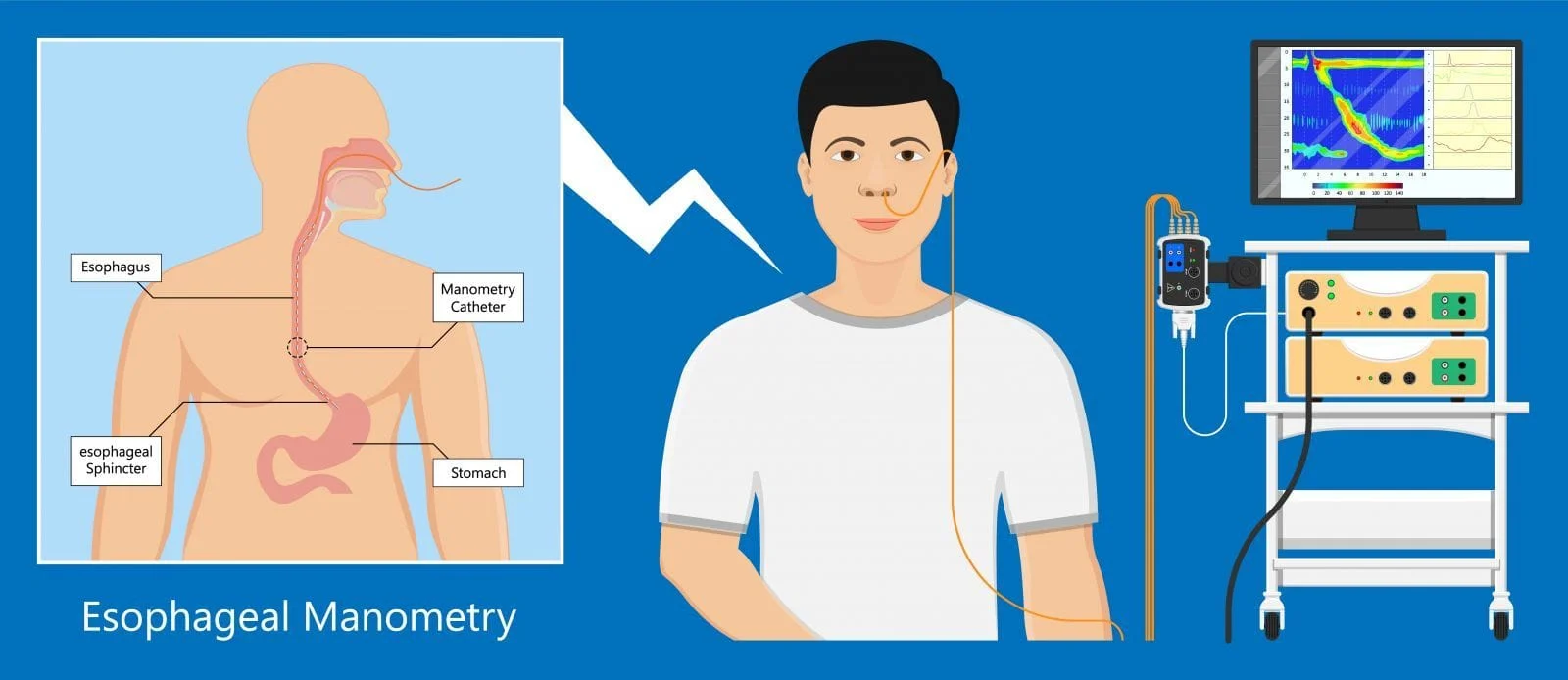
- Esophageal manometry is used to help determine if your lower esophageal sphincter (or LES) is functioning properly. This test involves swallowing a tube that measures the muscular contractions of your esophagus. It is usually reserved for more refractory cases of reflux.
What are the complications associated with GERD?
The vast majority of patients with GERD will NOT develop any serious complications, especially if it’s treated appropriately; however, serious complications can occur. Complications include:
- Peptic Ulcer Disease (PUD) or ulcers of the esophagus or stomach.
- Stricture, or a narrowing of the lining of the esophagus, caused by acid damage that scars and narrows the esophagus.
- Lung and throat problems — If acid is refluxed into the throat, the vocal cords can become inflamed and damaged, resulting in hoarseness, sore throat and cough. Acid inhaled into the lungs can result in aspiration pneumonia and permanent lung damage.
- Barrett's esophagus occurs when cells that normally line the lower esophagus are replaced with cells found in the stomach and intestines as a result of chronic acid exposure. Barrett’s esophagus increases your risk of developing esophageal cancer. As a result, people with Barrett's esophagus will require routine surveillance upper endoscopy to evaluate for changes in the lining of the esophagus suggestive of cancer.
- Esophageal cancer. The 2 main types of esophageal cancer are adenocarcinoma and squamous cell carcinoma. Barrett’s esophagus increases your risk of developing adenocarcinoma. Squamous cell carcinoma does not appear to be related to GERD.
How is GERD treated?
GERD is treated according to its severity.
Mild symptoms are often treated with dietary modifications and non-prescription medications.
Dietary and lifestyle modifications may include:
- Weight loss
- Elevate the head of your bed: Raising the head of the bed can be done with blocks of wood under the legs of the bed or a foam wedge under the mattress. It is not helpful to use additional pillows as this can cause an unnatural bend in your body that actually increases pressure on your stomach, worsening acid reflux.
- Avoid food triggers.
- Avoid Excessive caffeine, chocolate, alcohol, peppermint, and fatty foods
- Avoid citrus-based foods and tomato-based products
- Avoid alcohol
- Avoid tobacco: Saliva helps to neutralize refluxed acid, and smoking reduces the amount of saliva in the mouth and throat. Smoking also lowers the pressure in the lower esophageal sphincter and provokes coughing, causing frequent episodes of acid reflux in the esophagus.
- Avoid foods that relax the lower esophageal sphincter and thereby promote acid reflux (ex. Peppermint and caffeine).
- Avoid eating late at night– Lying down with a full stomach may increase the risk of acid reflux. Avoid eating 3 hours prior to bedtime.
- Avoid tight fitting clothing – At minimum, tight-fitting clothing can increase discomfort, but it may also increase pressure in the abdomen, forcing stomach contents into the esophagus.
- Chew gum or use oral lozenges – Chewing gum or using lozenges can increase saliva production, which may help to clear stomach acid that has entered the esophagus.
Moderate to severe symptoms may be treated with a proton pump inhibitor like omeprazole (Prilosec), esomeprazole (Nexium), lansoprazole (Prevacid), dexlansoprazole (Dexilant), pantoprazole (Protonix), and rabeprazole (AcipHex).
The goal of treatment is to take the lowest possible dose of medication that controls symptoms and prevents complications. Long-term risks of PPIs may include an increased risk of gut infections, such as Clostridioides (formerly Clostridium) difficile (C. diff), or reduced absorption of minerals and nutrients.
Surgical treatment is occasionally used for refractory cases and in patients with large hiatal hernias or other contributing conditions.
DISCLAIMER: PLEASE READ CAREFULLY
The information on this website is to provide general guidance. In no way does any of the information provided reflect definitive medical advice and self diagnoses should not be made based on information obtained online. It is important to consult a best in class gastroenterologist regarding ANY and ALL symptoms or signs as it may a sign of a serious illness or condition. A thorough consultation and examination should ALWAYS be performed for an accurate diagnosis and treatment plan. Be sure to call a physician or call our office today and schedule a consultation.