What is Barrett’s Esophagus?
Barrett’s Esophagus is a precancerous condition affecting the lining of the esophagus, the muscular tube that carries food and liquids from the mouth to the stomach.
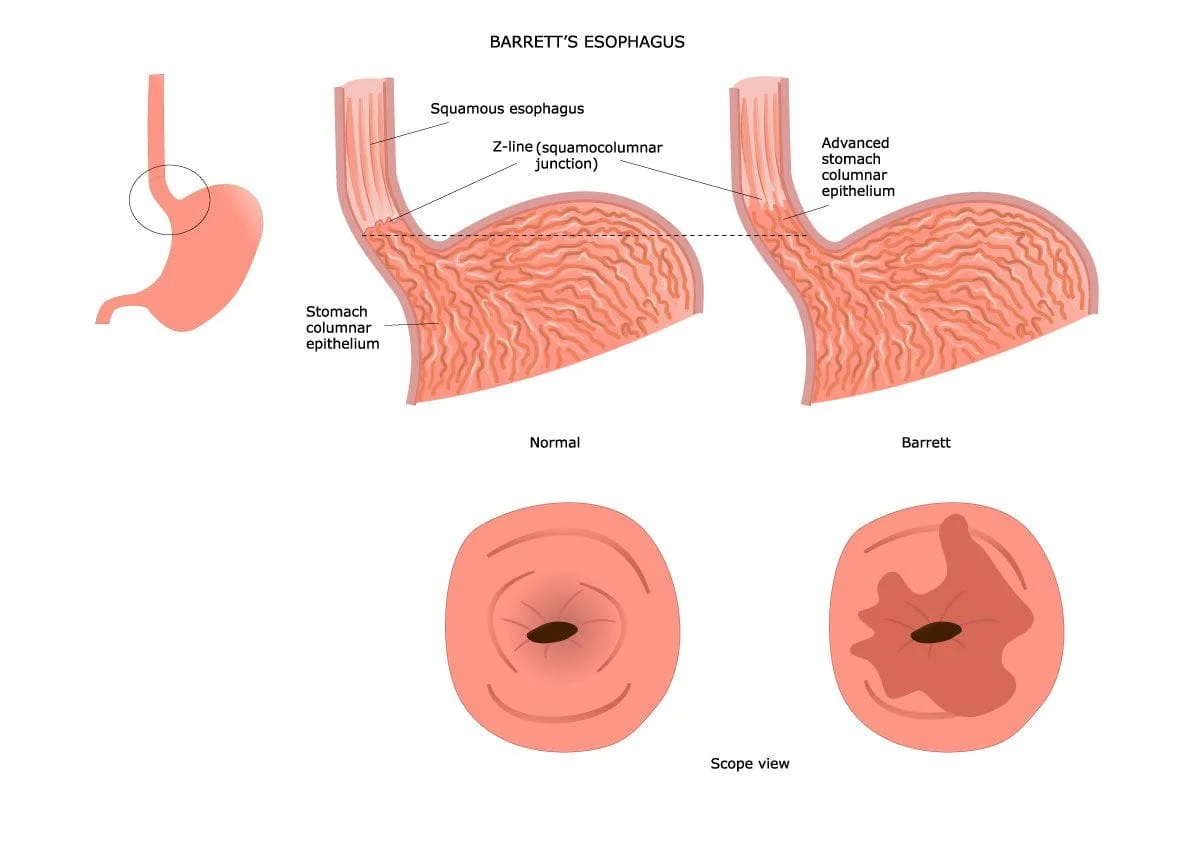
In Barrett’s Esophagus, normal healthy tissue lining the esophagus is replaced with abnormal tissue more similar in appearance to the lining of the intestines or stomach, a process known as “intestinal metaplasia”.
The inner lining of the esophagus is called the mucosa. Normally, the mucosa of the esophagus appears smooth and pink in color and is lined with flat cells that look similar to fish scales when viewed under a microscope. Medical professionals call these flat cells “squamous epithelium”. In Barrett’s esophagus, the esophageal mucosa starts to take on a salmon-colored appearance. An abnormal or “metaplastic” change in the cells lining the lower portion of the esophagus (the part closest to the stomach) occurs from normal squamous epithelium to simple columnar epithelium interspersed with goblet cells. These abnormal cells appear more like columns rather than flatfish scales. Physicians call this cellular change “specialized intestinal metaplasia”. Intestinal metaplasia can develop in any place where squamous mucosa normally exists, so it is not necessarily specific to the condition of Barrett’s Esophagus; however, when intestinal metaplasia replaces the squamous mucosa of the esophagus it is referred to as Barrett’s Esophagus.
What causes Barrett’s Esophagus?
Barrett’s Esophagus is believed to occur due to an adaptation of the cells lining the esophagus to chronic acid exposure from reflux esophagitis or gastroesophageal reflux disease (GERD). In a sense, Barrett’s Esophagus can be thought of as a flawed protective mechanism. The esophagus is not meant to withstand a significant amount of acidity, unlike the stomach and small intestine, structures that both play a role in the chemical digestion of foods (or the breakdown of foods by the action of chemical agents such as enzymes, acids, and bile). The esophagus is merely a muscular transport tube that pushes food from your mouth into your stomach. It’s only designed for this purpose, not to withstand high levels of acidity.
At the junction of the esophagus and the stomach, there is a muscle that opens and closes so that food can enter the stomach but not return back up into the esophagus. Sometimes this muscle, known as the lower esophageal sphincter (or LES), doesn’t work properly and stomach contents push back up into the esophagus. This is what happens in the case of gastroesophageal reflux disease or GERD. When the esophagus is chronically exposed to acid, esophageal mucosal cells start to look more like the cells lining the stomach and small intestine, cells designed to withstand acidity. This occurs as a last-ditch effort to protect the esophageal mucosa from the damage caused by continuous exposure to high levels of acidity. Unfortunately, these new and abnormal cells aren’t supposed to be found in the esophagus and their presence places a person at increased risk for esophageal cancer.
So Barrett’s Esophagus increases my risk for developing Esophageal Cancer?
Yes. People who have Barrett’s Esophagus have a small but increased risk compared with the general population for developing a specific type of esophageal cancer known as esophageal adenocarcinoma, a type of cancer that is often deadly.
The risk of esophageal adenocarcinoma in people with Barrett’s Esophagus is roughly 0.5% per year. Typically, precancerous cells (or dysplastic cells) will appear in Barrett’s tissue before frank carcinoma develops.
Dysplastic changes are divided into 2 grades based on how abnormal the cells appear under a microscope. These classifications are low-grade dysplasia and high-grade dysplasia. Patients with high-grade dysplasia have a risk of developing esophageal cancer as high as 10% per year or greater. Therefore, once a diagnosis of Barrett’s esophagus is made, patients are monitored closely with routine surveillance upper endoscopy (or EGD) to screen for esophageal cancer and other dysplastic changes in the cells lining the esophagus so that these changes can be identified and treated earlier on before frank cancer develops.
How is Barrett’s Esophagus Diagnosed?
A diagnosis of Barrett’s Esophagus is made by upper endoscopy through direct visualization of the affected tissue, and biopsy or microscopic evaluation of tissue samples taken during the procedure. Endoscopy and biopsy are the gold standard for diagnosis of Barrett’s Esophagus.
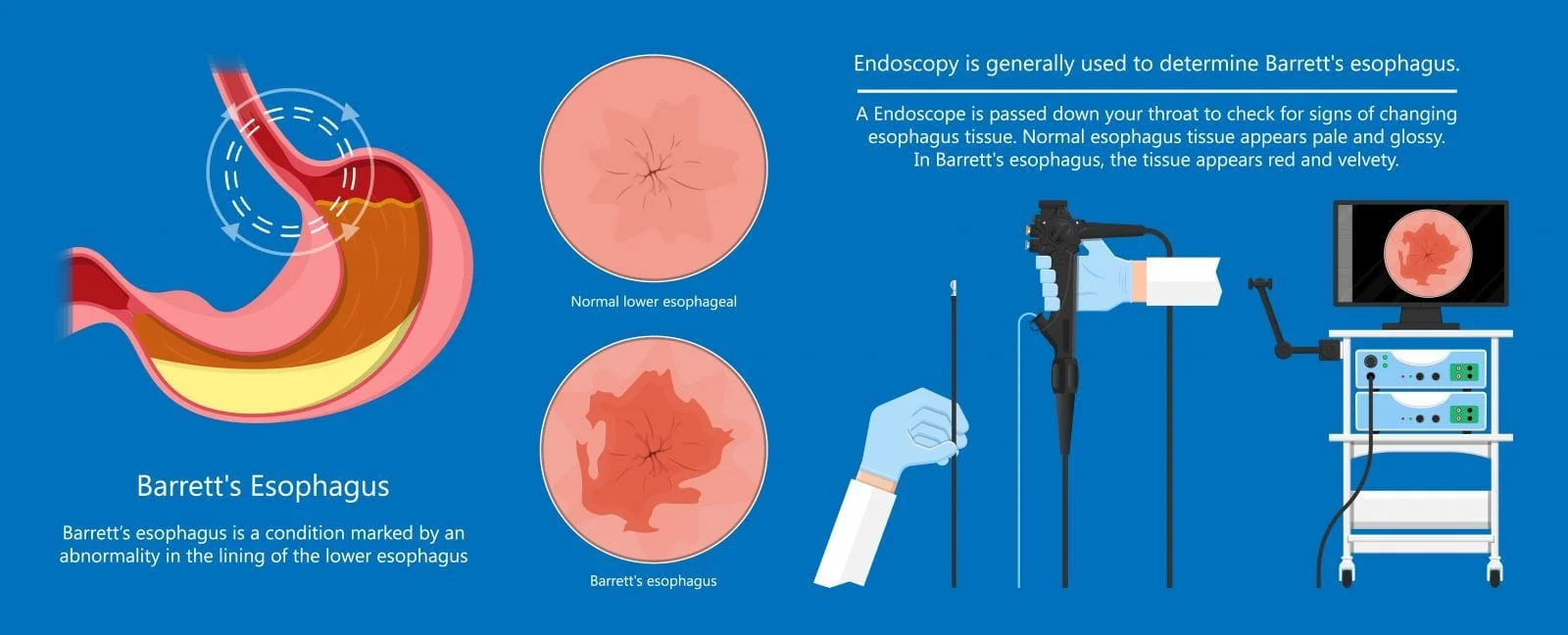
An upper GI endoscopy, also known as an Esophagogastroduodenoscopy, or EGD, is performed at an outpatient surgical center, or at the hospital, under light anesthesia. Dr. Sinha will carefully feed an endoscope with a light and camera attached to it through your mouth, down your esophagus, and into your stomach and duodenum, the first part of your small intestine. She will directly inspect the tissue of your upper gastrointestinal tract and take multiple biopsies, or small samples of tissue, from the lining of your lower esophagus or any other areas that appear irregular. A pathologist will then examine the tissue that she has sampled under a microscope to confirm or rule out the diagnosis of Barrett’s Esophagus. Diagnosis can be difficult because the condition does not affect all of the linings of your esophagus. Therefore, Dr. Sinha will take biopsy samples from at least eight different areas of the lining of your esophagus to assess for the condition.
She will use two main criteria to make the diagnosis of Barrett’s Esophagus: a salmon color to your esophagus and other visual changes suggestive of the disease, and cellular changes seen in the samples of tissues or biopsies taken during your EGD. These cellular changes include intestinal metaplasia and the presence of Goblet cells, a type of cell usually present in the intestinal mucosa. Goblet cells are one of the hallmark findings in Barrett’s Esophagus.
If you are diagnosed with Barrett’s Esophagus the condition will be classified as a short segment (meaning less than 3 cm of Barrett’s mucosa), long segment (4-10cm of Barrett’s mucosa) or very long segment (more than 10cm) depending upon how long the affected area of the esophagus is.
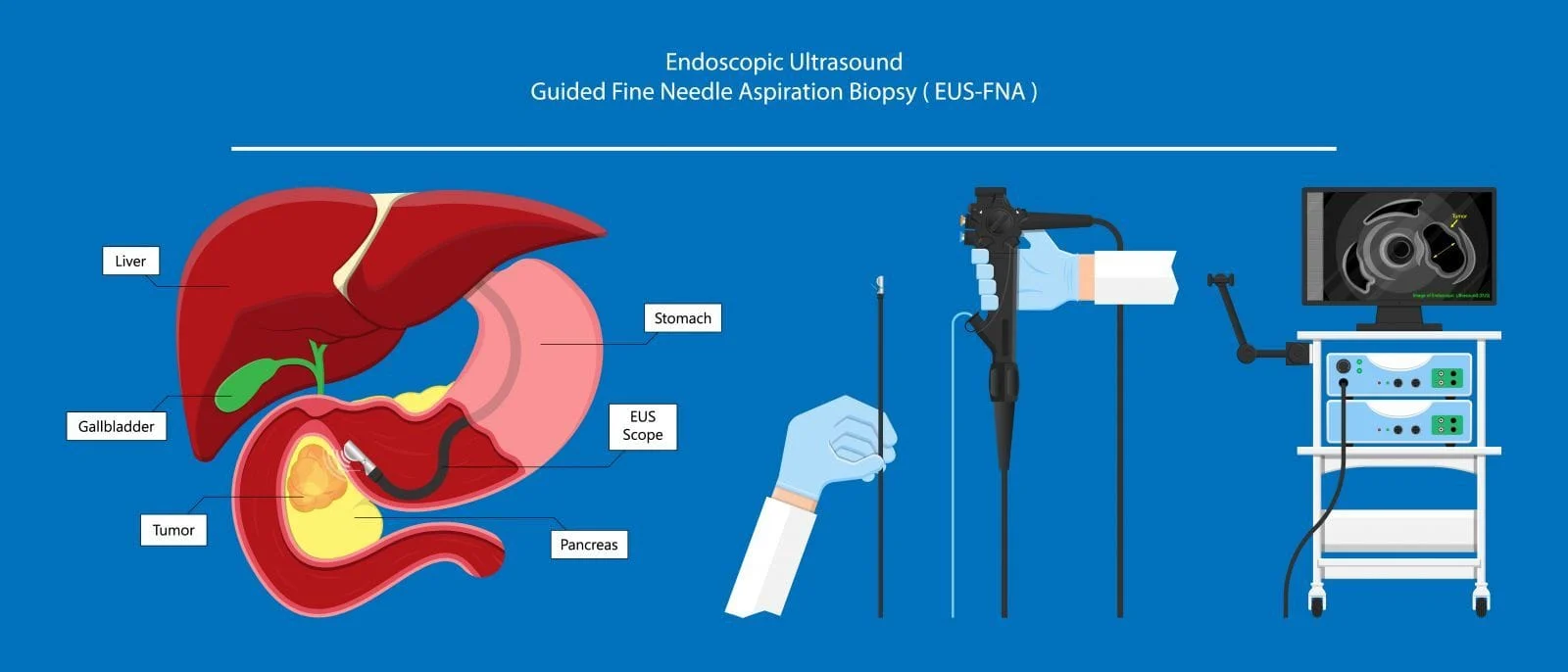
Sometimes further testing may be needed to assess the extent of the disease including Endoscopic Ultrasound (or EUS), a minimally invasive procedure where a special endoscope uses high-frequency sound waves (or ultrasound) to produce detailed images of the lining and walls of your digestive tract and chest, nearby organs such as the pancreas and liver, and lymph nodes.
How common is Barrett’s Esophagus?
Estimates of the prevalence of Barrett’s Esophagus in the general population vary widely depending upon the population studied and the criteria used to make the diagnosis, but in general is affects roughly 0.4-20% of the general population. About 21% of patients with uncomplicated reflux symptoms are thought to be affected.
It is 2-3 times more common in men than women, and Caucasian men are more likely to be affected than any other race. The average age of diagnosis is 55 years of age.
What are the risk factors for Barrett’s Esophagus?
Risk factors include:
- Being male,
- Being over 50 years of age,
- Being a former or current smoker,
- Being obese,
- Having a family history of Barrett’s Esophagus, and
- Having a personal history of longstanding reflux symptoms, chronic heartburn, or gastroesophageal reflux disease (or GERD)
- GERD is a condition where your stomach contents flow back up into your esophagus and cause bothersome symptoms. Refluxed stomach acid irritates the lining of your esophagus, potentially damages cells, and causes heartburn. Roughly 10-15% of people with GERD go on to develop Barrett’s Esophagus.
What are the symptoms of Barrett’s Esophagus?
While Barrett’s Esophagus itself doesn’t produce symptoms, Barrett’s patients will often have:
- Chronic heartburn,
- Reflux, and/or
- GERD.
- Common symptoms of GERD include:
- A burning sensation in the chest (or heartburn) usually after eating and often worse at night or when lying down,
- Belching,
- Nausea,
- Regurgitation of food or sour liquid,
- A sour or bitter taste in the back of the throat,
- Hoarseness, dry cough,
- Chest pain,
- Difficulty swallowing,
- The sensation of a lump in your throat, and
- Bad breath or tooth decay.
- Common symptoms of GERD include:
How is Barrett’s Esophagus treated?
Treatment options for Barrett’s Esophagus are dependent upon the extent of the condition and dysplasia but include:
- Medications for GERD such a proton pump inhibitors® (or PPIs).
- Endoscopic ablative therapies,
- Endoscopic mucosal resection and
- Surgical resection.
Medications: Treatment options for medications include acid-suppressing medications like proton pump inhibitors® (PPIs). These medications prevent further damage to the esophagus and in some cases heal existing damage. They do come with potential side effects including (but not limited to) headache, diarrhea, constipation, abdominal pain, gas or flatulence, fever, vomiting, nausea, and rash. PPIs may increase the risk for Clostridium difficile (C. diff) infection. High dose and long-term use may increase your risk for osteoporosis-related fractures as well.
Other Treatment options: Endoscopic ablative therapies use different techniques to destroy the abnormal or dysplastic changes in your esophagus. Ablation destroys damaged esophageal cells and prevents the further progression of Barrett’s esophagus. Each type of ablation treatment uses heat or cold energy to target precancerous esophageal cells while preserving healthy esophageal tissue. After ablative therapies, ideally, your body will begin making normal esophageal cells.
What if I’m diagnosed with Barrett’s Esophagus? Will I need any type of follow up or surveillance?
Periodic surveillance endoscopy (or EGD) is recommended for all patients to watch for cellular changes suggestive of worsening disease or the development of cancer. After an initial diagnosis of Barrett’s Esophagus, you will be advised to have a repeat EGD in 6-12 months for surveillance depending upon the extent of your condition. Thereafter, surveillance EGD is recommended at least every 3 years, if not more frequently, depending upon the extent of your disease.
What can I do to reduce my risk of developing Barrett’s Esophagus?
Your risk for developing Barrett’s Esophagus may be decreased if you’ve ever had an infection with H. pylori, a bacterium commonly associated with the development of Peptic Ulcer Disease. Researchers are unsure why or how H. pylori might protect the esophagus against Barrett’s Esophagus.
Other factors that may decrease your risk for the development of Barrett’s Esophagus include a diet high in fruit, vegetables, and certain vitamins such as vitamins C, E, selenium, and carotenoids.
The biggest thing you can do is follow anti-reflux measures, avoid triggers that result in reflux or heartburn symptoms, and discontinue smoking if you are a smoker.
What dietary or lifestyle modifications are recommended?
Dietary and lifestyle changes that can help to further prevent the progression of Barrett’s esophagus include:
- Treating any underlying GERD or reflux symptoms,
- Decreasing fatty foods,
- Eating smaller, more frequent meals, instead of three large meals,
- Avoiding chocolate, coffee, peppermint, greasy or spicy foods, tomato based products, acidic foods, citrus fruits, and alcoholic beverages,
- STOP smoking, and
- Lose any excess weight.
DISCLAIMER: PLEASE READ CAREFULLY
The information on this website is to provide general guidance. In no way does any of the information provided reflect definitive medical advice and self diagnoses should not be made based on information obtained online. It is important to consult a best in class gastroenterologist regarding ANY and ALL symptoms or signs as it may a sign of a serious illness or condition. A thorough consultation and examination should ALWAYS be performed for an accurate diagnosis and treatment plan. Be sure to call a physician or call our office today and schedule a consultation.