Hormonal Triggers of GI Disease including PCOS and Endometriosis
PCOS, Endometriosis and Other Hormonal Triggers for GI Symptoms
Hormonal fluctuations related to the menstrual cycle, certain gynecological and endocrine disorders, and menopause can contribute to GI symptoms like gas, bloating, diarrhea, constipation, and slowed digestion in women. Hormonal imbalances and fluctuations can also aggravate and exacerbate underlying GI disorders like IBS and IBD.
While we do NOT treat gynecological disorders at Hunterdon Digestive Health Specialists (we are a Gastroenterology practice ), and ALL gynecological symptoms and disorders should be managed by a trained OBGYN or other certified professional, estrogen, progesterone, and other hormones can significantly affect GI symptoms and underlying GI diseases like IBS and IBD, which we DO treat. We can help you manage these associated GI symptoms and conditions.
Sometimes understanding why your symptoms occur, and why they occur when they occur, can be empowering to you, allowing you to better manage your day-to-day life and experience an overall better sense of well-being.
What gynecological and endocrine disorders can contribute to GI symptoms?
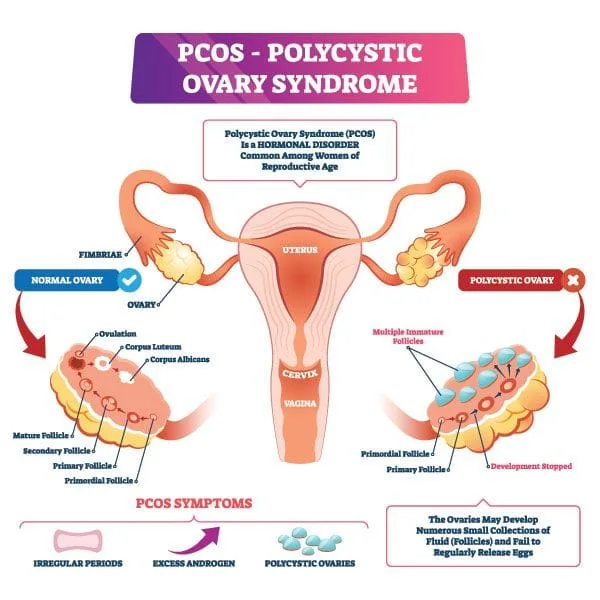
1. Polycystic ovary syndrome (or PCOS)
PCOS is a common hormonal disorder that affects women of childbearing age. With PCOS the ovaries produce abnormal amounts of androgens, or male sex hormones usually present in women in small amounts. Testosterone is the most common androgen that most of us are familiar with. Some women will have small fluid-filled cysts on their ovaries, which is where the name “polycystic” or “many cysts” comes from; however, this is not required for a diagnosis of the disease. Women with PCOS often have irregular menstrual cycles, and fail to ovulate regularly.
What causes PCOS?
The exact cause of PCOS is unknown.
Many women with PCOS have insulin resistance. Insulin is a hormone produced by the pancreas that allows our cells to use glucose (or sugar). After you eat, your blood sugar (or glucose) levels rise. This rise in glucose triggers your pancreas to release insulin into your bloodstream. Insulin travels throughout the blood to your body's cells. It tells the cells to open up and let glucose in. Once inside, the cells convert glucose into energy, or store it for later use. Without insulin, your body can't use or store glucose for energy. Instead, the glucose stays in your blood, and a condition known as diabetes can follow.
With insulin resistance your cells don’t respond to insulin like they used to. Your pancreas is still capable of producing insulin, and in fact it ends up producing a LOT of insulin, but your cells resist or ignore the signals from insulin to open up and let glucose in. Over time, cells need more and more insulin to actually take in glucose and use it for energy. As a result, your pancreas keeps producing more and more insulin thinking that your cells need it. Excess insulin builds up in the body, which causes the ovaries to produce abnormally high levels of androgens (or testosterone), resulting in symptoms of hirsutism (unwanted facial and body hair) and acne. Higher androgen levels also cause problems with the menstrual cycle, ovulation, and fertility. Obesity itself, apart from PCOS, increases insulin levels and make PCOS symptoms worse.
PCOS may have a genetic component. Research suggests that women with PCOS have altered levels of some inflammatory markers like C-reactive protein, which may reflect a state of chronic low-grade inflammation. Inflammation is believed to be a driving force in the development of many metabolic problems associated with PCOS such as insulin resistance, Type 2 Diabetes, and non-alcoholic fatty liver disease.
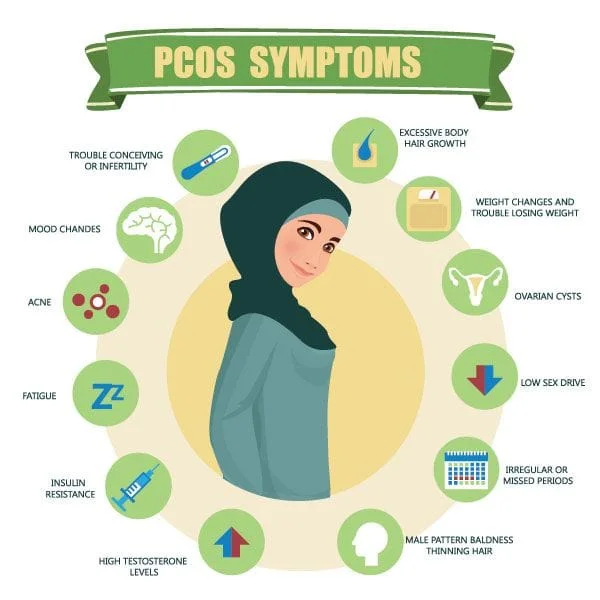
What are the symptoms of PCOS?
Again, ALL gynecological concerns should be discussed with your OBGYN and/or Primary Care Physician; however signs and symptoms may include:
Cystic ovaries
Irregular menstrual cycles
Heavy periods
Hirsutism (or unwanted facial and body hair in areas where women don’t typically have hair)
Hair loss
Acne or oily skin
Thick, dark, velvety patches of skin under your arms, breasts, on the back of your neck, and in the groin known as acanthosis nigricans.
Difficult sleeping
Headaches
Trouble getting pregnant or infertility
Weight gain
Elevated cholesterol
Elevated blood sugar or insulin levels
What are the complications of PCOS?
Complications may include:
Infertility
Gestational diabetes
Nonalcoholic fatty liver disease (NAFLD) and Nonalcoholic steatohepatitis (or NASH), which NASH being liver inflammation and damage to the liver caused by a buildup of fat in the liver.
Metabolic syndrome (or a cluster of conditions including high blood pressure, abnormal blood glucose levels, excess body fat around the waist, and abnormal cholesterol or triglyceride levels)
Type 2 diabetes
Abnormal menstrual cycles and bleeding
Hirsutism, and
Obesity
How is PCOS related to GI disease?
Women with PCOS have a higher prevalence of IBS compared with those not affected by PCOS; however, a direct correlation between the two diseases has not yet been identified.
PCOS is associated with excess androgen (or testosterone) levels, insulin resistance, and inflammation, ALL of which can alter bowel function and contribute to GI conditions like IBS and Small Intestinal Bacterial Overgrowth (or SIBO).
SIBO is defined as excessive or abnormal bacteria present in the small intestine. It remains a poorly understood disease; however, is strongly linked with IBS. Overgrowth of bacteria in the small intestine may result in microscopic inflammation in the small intestine and malabsorption of nutrients from the small intestine.
SIBO can be caused by a number of factors, but in relation to PCOS, insulin resistance can affect stomach acid (or HCL) levels. HCL is our first line defense against foreign invaders to the GI tract. It also helps us to chemically digest our food. If we don’t have the right balance of stomach acid we may be more prone to certain GI infections and SIBO. An imbalance of HCL may also inhibit us from properly digesting our foods. Additionally, hormonal imbalances associated with PCOS are known to alter how fast food moves through the GI tract, causing diarrhea or constipation, which can both contribute to the development of SIBO. An imbalance of bacteria in our small intestine, as seen in SIBO, can cause inflammation, which can potentially make PCOS symptoms worse. Inflammation exacerbates insulin resistance, which causes the ovaries to produce excess testosterone, which disrupts the menstrual cycle, and prevents ovulation.
PCOS is significantly associated with a high risk of developing Nonalcoholic fatty liver disease (or NAFLD) and Nonalcoholic steatohepatitis (or NASH).
Nonalcoholic fatty liver disease (NAFLD) is a condition where excess fat is stored in the liver. It is NOT caused by heavy alcohol use, and there is not inflammation or damage to the liver associated with this excess fat build-up.
Nonalcoholic steatohepatitis (NASH); however, IS LIVER INFLAMMATION and DAMAGE to the liver caused by a buildup of fat in the liver.
Regarding PCOS patients, research suggests the higher your androgen or testosterone levels the greater your risk for developing these conditions.
Fatty Liver screening is crucial in PCOS patients.
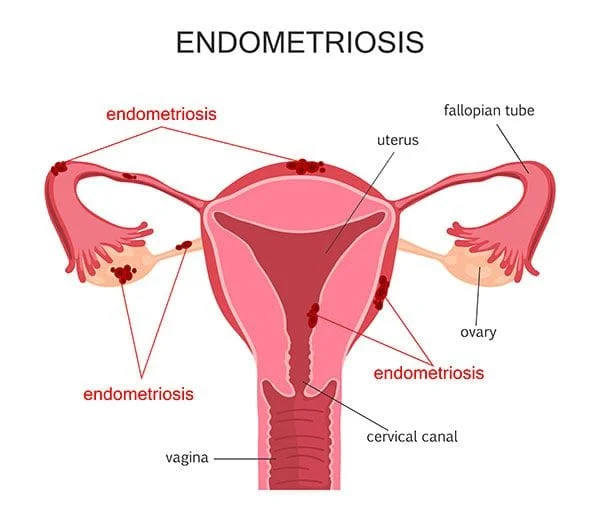
2. Endometriosis
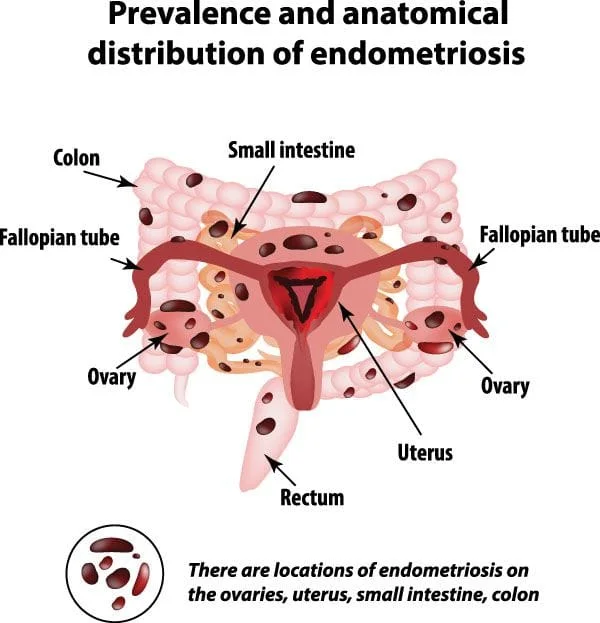
Endometriosis is a common gynecological condition, affecting roughly 10% of women where tissue similar to the tissue that forms the lining of your uterus grows OUTSIDE of your uterus. The lining of your uterus is known as the “endometrium”, so “endometriosis” is referring to this type of uterine tissue.
With Endometriosis, endometrial (or uterine) tissue may abnormally grow on your ovaries, in your bowel, and in the tissues lining your pelvis.
The hormonal changes associated your menstrual cycle can affect this misplaced tissue and cause these areas to become inflamed and painful. Just like your uterine lining grows, thickens, and sheds each month with your menstrual cycle, this abnormally placed tissue will do the same. Over time, scar tissue, adhesions and problems with fertility can occur
What are the symptoms of Endometriosis?
Again, ALL gynecological concerns should be discussed with your OBGYN and/or Primary Care Physician; however signs and symptoms may include:
Pelvic pain
Painful periods
Pain in the lower abdomen or back
Cramps
Heavy or irregular periods
Spotting
Infertility
Pain with intercourse,
Pain with bowel movements
How is Endometriosis related to GI disease?
Endometriosis can be found directly in the bowel, although this only occurs in a small percentage of patients. Still, even when endometriosis does not occur directly in the GI tract, it can cause GI symptoms, and women with Endometriosis will OFTEN experience GI symptoms. They may suffer from abdominal pain, constipation, diarrhea, painful bowel movements, gas and bloating, intestinal cramping, increased urgency to go to the bathroom, a sensation of incomplete emptying, rectal pain or spasms, rectal bleeding, nausea, and/or vomiting. Often GI symptoms will be more pronounced just before or during menstruation. This is because inflammatory markers like prostaglandins from the endometriosis implants released around the time of menstruation can cause not just the uterus but also the bowel to contract, resulting in diarrhea and cramping. While endometriosis is not an autoimmune disease like Inflammatory Bowel Disease (or IBD), it has been linked to several other autoimmune conditions. Because of this connection to autoimmune disease, researchers are looking into whether or not there may be an autoimmune connection between endometriosis and IBD. As many as 8% of endometriosis patients with bowel symptoms may eventually go on to be diagnosed with IBD including Crohn’s Disease and/ Ulcerative Colitis.
Endometriosis is often treated with hormonal therapies like oral contraceptives, which some research has suggested might increase one’s risk for developing IBD and other associated GI conditions like gallbladder disease. The connection between the IBD and endometriosis is not well understood or define; nonetheless, if you have GI concerns please contact our office for a comprehensive evaluation of your symptoms to avoid delayed care, missed diagnoses, and poor outcomes!
Why do my GI symptoms seem to follow a cyclical pattern related to my menstrual cycle, or be worse with PMS?
*** While we do NOT treat gynecological disorders and ALL gynecological symptoms and disorders should be managed by your OBGYN or another trained professional, estrogen, progesterone, and hormonal imbalances can significantly affect GI symptoms and underlying GI diseases like IBS and IBD, which we do treat.
We believe that understanding why your symptoms occur, and why they happen when they do, can be empowering to you, allowing you to be a better advocate for your own health, to seek out the appropriate specialty care, and to manage your day-to-day symptoms and overall life better.
Hormonal fluctuations related to the menstrual cycle can cause many symptoms including: fluid retention or swelling, gas, bloating, diarrhea, constipation, and slowed digestion.
An increase in GI symptoms around the time of menstruation seems to correlate most with declining or low levels of ovarian hormones, suggesting that estrogen and progesterone withdrawal play a role in symptoms.
When estrogen levels are high, women tend to retain more water resulting in bloating.
When progesterone levels are high, like during the 2nd half of your menstrual cycle, GI transit time can be delayed, resulting in food moving more slowly through your GI tract, causing symptoms of constipation and bloating.
When progesterone levels drop and menstrual bleeding begins, many women notice an increase in bowel activity resulting in diarrhea, increased gas, and bloating.
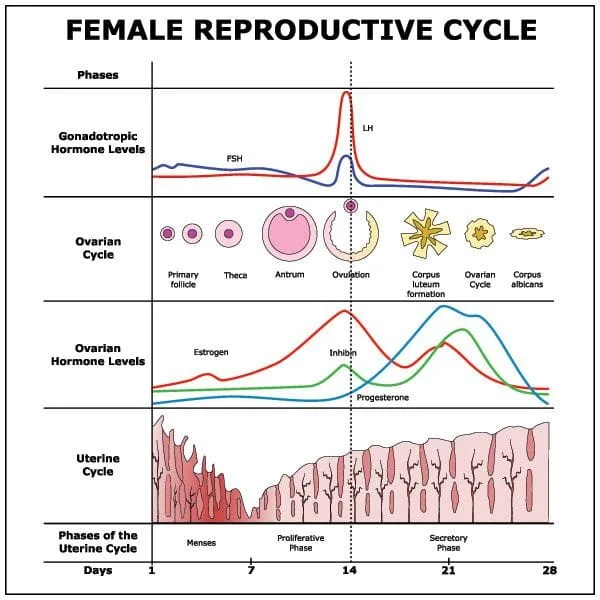
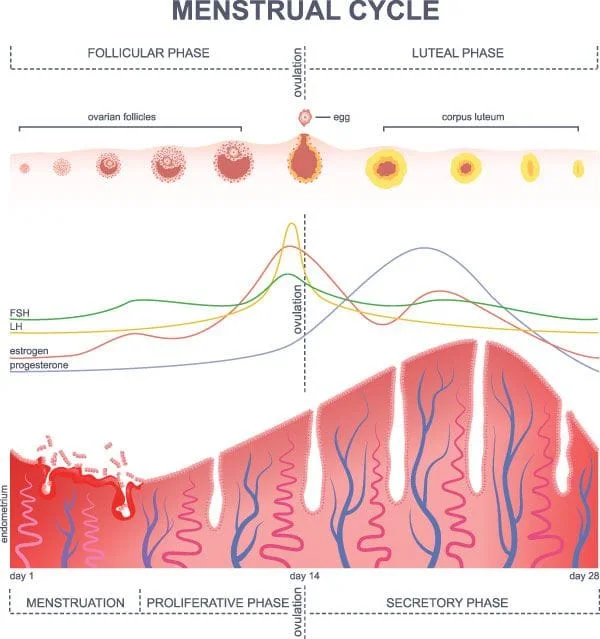
The menstrual cycle has 4 phases. Overall length can vary and typical length is often described as 28 days, although only a portion of the population actually follows a true, consistent, 28-day menstrual cycle. The 4 phases of the menstrual cycle include:
Menses (roughly days 1-5): If you’re not pregnant, you shed the lining of your uterus during menstruation. Here, estrogen and progesterone levels will typically be at their lowest.
Follicular Phase: This is the first half of your menstrual cycle, roughly days 1-14, up until ovulation. During this phase estrogen is produced from sacs that contain your eggs, called follicles. Estrogen levels rise during the follicular phases causing the lining of your uterus (or endometrium) to thicken in preparation for pregnancy. About halfway through this phase (just as your period is ending) one follicle in one of your ovaries will be the largest of all of the follicles. This follicle becomes the “dominant follicle” and prepares to be released at ovulation. Near the end of this phase, your estrogen levels peak, triggering the anterior pituitary gland in your brain to release two hormones: a large surge of luteinizing hormone (LH), and a smaller surge of follicle stimulating hormone (FSH). The surge of these hormones is what triggers ovulation. Just before ovulation the dominant follicle stops producing estrogen and estrogen levels drop off.
Ovulation (roughly day 14): This is when the egg is released from the dominant follicle, and pregnancy can occur if sperm is present in the female reproductive tract.
Luteal Phase (roughly days 15-28): Where the dominant follicle was, now a new hormone-producing structure called the corpus luteum forms from the walls of the follicle. The main function of the corpus luteum is to produce hormones (lots of progesterone, and some estrogen, too), in order to prepare the uterus for pregnancy. If an egg is not fertilized and implanted, the corpus luteum will stop producing progesterone and estrogen roughly around days 24-28, and the levels of both of these hormones will quickly drop off, triggering the start of menstruation. During the late luteal phase, you’re most likely to experience bloating, constipation and/or diarrhea due to hormonal changes.
How can I manage my GI symptoms during my period?
First and foremost, ALL symptoms should be evaluated by a trained medical professional to avoid missed diagnoses, delayed care and poor outcomes. Some simple lifestyle and dietary modifications that may help include:
Avoid trigger foods. Keep a food diary to identify food triggers and avoid these as much as possible.
Drink plenty of fluids. Keep hydrated. This is your best defense against constipation.
Get enough sleep. This will help to keep your immune system strong and healthy.
Get plenty of exercise. Again this will help your immune health but also help with digestion. Regular exercise helps to keep food moving along your GI tract and prevent constipation. Always consult with a medical professional first before starting any exercise program.
Avoid gas-producing foods like beans, vegetables in the cabbage family, and dairy.
Avoid carbonated beverages, processed foods, simple sugars, and artificial sugars like those found in diet products. Read your food labels because often these artificial sugars are snuck into foods that we might think are otherwise good for us, like yogurts.
Contact Us
Our Location
Find us on the map
Hours of Operation
Our Regular Schedule
Hunterdon Digestive Health Specialists
Monday:
8:00 am-6:00 pm
Tuesday:
8:00 am-7:00 pm
Wednesday:
8:00 am-5:00 pm
Thursday:
8:00 am-6:00 pm
Friday:
8:00 am-7:00 pm
Saturday:
*Contact office to confirm Saturday hours and availability*